
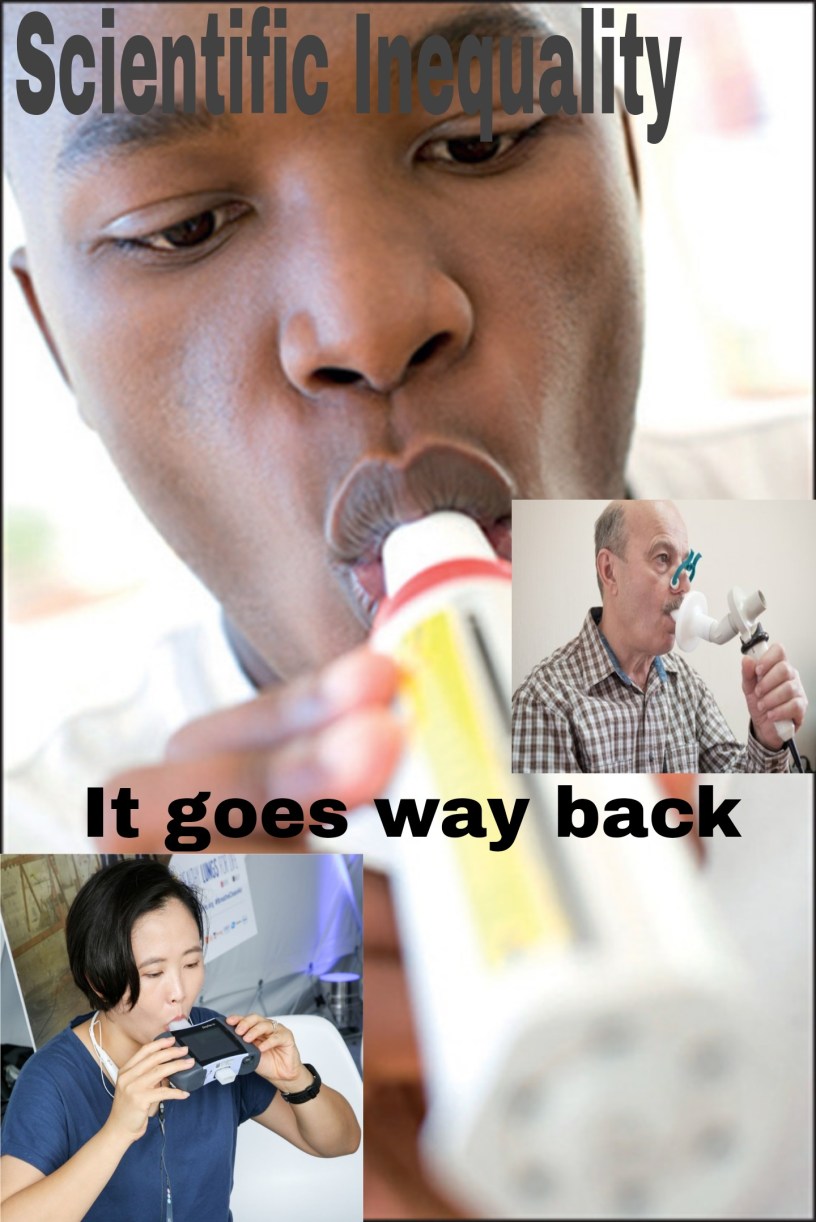
Starting a new series of on a look into the past on how science and politics intersect. So like the titles says, we are about to get into a touchy subject. Let’s learn about the Spirometer.
As a question have you or someone you known ever used a spirometer? Honestly I had no idea what the hell a spirometer was and unknowingly didn’t realize I had used one in the past. In fact, many of my family members have used it and given the history of the development of this science and medical device, I’m feeling a bit cheated. In fact, as a scientist and a black man I am straight up offended. A lot of the the information will be following the work of Dr. Lundy Braun who published a Article titled “Race, ethnicity and lung function: A brief history” that chronicles the history of the spirometer and helps validate a lot of my sentiments.
Over the past century the spirometer has been used to determine the lung function of a person. It works by breathing into a tube that looks like the attachment to a vacuum head and can measure how much air you inhale and exhale using a piston. The piston is moved forcibly by your breath and it can even determine the rate of which you can exhale. Pretty objective measurement right? Until of course humans enter the playing field. In a effort to explain the variability found within certain populations many scientists and physicians have royally screwed this one up.

In a effort to “standardize” the results across the globe often times a race correction factor is applied. In the United States (US), spirometers use either race correction factors of 10% to 15% for individuals labelled ‘black’ and 4% to 6% for people labelled ‘Asian’, or population-specific standards, usually those derived from the third US-based National Health and Nutrition Examination Survey for ‘Caucasians’, African Americans and Hispanics. In other words, the assumption is that the lungs of black people, and Asians aren’t as strong as our white counterparts. I guess they never watched a Kenyan marathon runner or Usain Bolt? On another note why is it everytime something is standardized it means more people of color are left behind? I digress, my blood pressure is getting to high….yet another health diagnosis for black people.
So how did the Spirometer get this race correction factor? Well look no further than what else…….slavery. In Thomas Jefferson’s Notes on the state of Virginia, he wrote about lung differences between slaves and white colonists. Among the many physical distinctions that Thomas Jefferson described to justify the condition of slaves in the republic, one was “a difference of structure in the pulmonary apparatus”. In other words, the slaves had weak lungs but not weak enough to farm, clean, cook, tend to the animals, or God knows what else. Of course like many racist things this thought continued thru time.
Interest in the spirometer increased significantly in 1840 after John Hutchinson a London based physician (sometimes the racism is imported) published several studies describing the technical features of the spirometer and its potential applications for monitoring the fitness of the police and armed forces, and life insurance applicants and for diagnosing tuberculosis. However, there was a issue that Hutchinson ran into regarding the Spirometer. Even though it would be nice to see a correlation of height to lung capacity there were several discrepancies that couldn’t be compensated for and needed to be explained.

Knowledge of the spirometer grew into Germany and particularly the American south with plantation owners, physicians, and slaveholders. (Yup it’s about to go there). Enter Samuel Cartwright who as a slaveholder, and physician decided to interpret Jefferson’s framework of a spirometer to test the lung capacity of slaves and whites. According to Cartwright, “the deficiency in the negro” was “20 per cent”. Defining difference as ‘deficiency’, Cartwright established race as a key organizing principle of lung function measurements in the US. (Insert reference). Yeah there isn’t much else I can say on that but WTF!!!
Jefferson’s work expanded even further when racial examination expanded to the North in 1964 under the leadership of Benjamin Apthorp Gould. Gould was commissioned by the US government to after the civil war to look at the differences in black and white soldiers and without any adjustment for height or age, or attention to working and living conditions of newly emancipated slaves, Gould reported that “full blacks” had lower lung capacity than “whites”. It all seems pretty scientific right? Well Frederick Hoffman thought so and as the heads of Prudential life insurance some 30 years later made the judgment that “the smaller lung capacity of the colored race is in itself proof of an inferior physical organism”. It’s almost like this racism is growing metastasizing one would say.
However this cancer was met with some resistance in which intellectuals like WEB DuBois and Kelly Miller wrote scathing critiques against Hoffman’s assessment. Unfortunately to little avail. In the 1920s eugenics became and even larger endeavor and enterprise globally. In most studies, whites had higher lung capacity than blacks, Chinese or Indians; explanations for findings centred on innate difference. For example, Wilson and Edwards published the first set of spirometry-based lung function standards according to race in 1922, speculating that difference could be due to “a possible racial factor”. By 1925, JE Myers published his reference handbook for clinicians, in which he reported differences among whites, blacks, Chinese and Filipinos as unquestioned fact See that snowball getting bigger?

So how does this relate to today? Well glad you asked, in 1974 a collaboration between Charles Rossiter of the Pneumoconiosis Unit in South Wales and Hans Weill of Tulane Medical School in New Orleans, Louisiana produced a large proportion of the literature used an explanatory framework that emphasized innate or anthropometric difference. For the most part, researchers assumed racial identities to be straightforward. Or in other words assumed race explained the innate differences in lung capacity. However it would take researchers from the Apartheid South Africa to raise serious questions on the accounting of social conditions for the impact on the lives of the people who were examined. Unfortunately, like Debois these articles weren’t cited and became apart of the literature. It’s almost as if it’s systemic.
Conclusion
With that manufacturers of the spirometer have baked in a correction factor for race. Many medical professionals aren’t even aware of this and the ones who are often cite the same articles as fact. However as a complete scientist we have to understand the historical relevance and context of the study. That in fact science is performed by people who are biased and dare I say racist. The history of the spirometer points this fact out. Data is one thing but try to understand the full picture you just might be surprised.
